Doctor’s 35-hr shift on 8 bananas, a toilet in nearby cafe

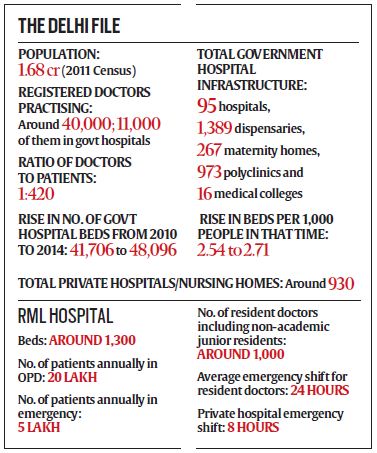
It’s 15 days after their strike ended, and the 32-year-old is back at work at Ram Manohar Lohia Hospital, located on the bustling Baba Kharak Singh Marg in Central Delhi. The hospital gets around 20 lakh patients annually in OPD, 5 lakh in emergency, and the PG resident in surgery is among its 1,000-odd resident doctors, including non-academic junior residents.
Today Dr M’s (name withheld to protect his identity) duty begins in the surgical emergency, and he arrives at 8.50 am, bolstered for the next 36 hours that will follow with a change of shirt, his copy of the Sabiston Textbook of Surgery, three packets of glucose biscuits, eight bananas and two bottles of water.
Dr M is happy today. He has had five continuous hours of sleep.
There are 45 patients in the surgical emergency ward, sharing a total of 20 beds. Two beds are empty — left for patients who may show up with grave emergencies. Two to three patients share most of the occupied beds; a couple of them have up to four.
Dr M and other senior residents begin their round checking on the patients admitted in the previous shift. The patients here are awaiting procedures, either because the operation theatre is not free or because essential pre-surgery investigation reports haven’t yet come in.
Dr M and a senior sort case sheets in decreasing order of priority. The emergency has a single major OT, shared between the departments of general surgery, gynaecology, paediatric surgery, burns and plastic surgery, ENT and opthalmology. And it is always occupied.
There is a minor OT but that is used for mostly sutures or cleaning of open wounds.
In his first round, Dr M does four catheterisations and changes canulas on six patients. Angry relatives of two patients, both awaiting prostrate surgery and sharing a bed, demand to know why their urine bags are leaking — it’s a common problem, the doctors pacify them.
In the next 24 hours of his duty in emergency, Dr M will do at least 500-600 cathetrisations and canula tweaks alone. In a private hospital ER, both these procedures are done by nurses.
Around 10 am, Dr M scrubs in for the first surgery of his shift. It is a 32-year-old abdominal tuberculosis patient who has been awaiting his turn in the OT for a week.
The surgery lasts five hours. A usual surgery in the emergency OT takes around two hours, and there is a restless crowd waiting outside by now. It’s nearly afternoon and no patient who has come this day has been admitted so far. Dr M is sent out to pacify the edgy relatives.
Dr M shouts out to a nurse that one of the “spider lights” — placed atop a surgery OT table — is not working again. The nurse, busy filling out the fast-depleting blood transfusion forms, barely listens.
Gobbling down two biscuits and a banana, Dr M braces himself for his next shift — at the desk — beginning 3.30 pm. Six chairs are placed around a normal-sized desk. Patients who report to casualty are divided into surgical, medicine and orthopaedic emergencies. Desk duty means reviewing an average of 50 cases in an hour to direct patients where they need to go — minor OT, major OT or admission.
Police bring in two patients who have been in a brawl — one has a cut below the eye, the other above. Dr M decides to handle the cut below the eyebrow himself, and assigns an intern to the second case. “How dare you put a junior doctor on my case? Is his vision more precious?” the other patient screams. Dr M tries to explain that a cut above the eye is far easier to stitch.
The lights in the minor OT are not working, and patient beds are placed along walls with regular house bulbs aligned to illuminate the room.
At 5 pm, Dr M shortlists a 26-year-old road accident victim with blunt trauma to his abdomen as the next surgical case. The family is reasonably well to do and agrees to get some pre-surgery essential tests done outside the hospital. These would take hours at the emergency ward. But when told that even a CT abdomen or a CECT abdomen — a radiological test to see the exact spot of the injury — was not available, the family erupts, hurling abuses at the junior doctors.
It is left to Dr M again to explain that only head CT is done in emergency. Meanwhile, the patient is slipping. Doctors decide against wasting any time and wheel him into the OT. They are used to waiving away protocols such as essential tests to save lives now.
It proves to be a case of spleen rupture. It takes two hours to remove the patient’s spleen.
As doctors start closing up the patient, Dr M is sent out to calm down a gynaecology resident who has been waiting for the OT for an emergency caesarean. Every two hours almost, the ward receives a caesarean case. Caesareans always get priority, with the principle brutally simple: it involves two lives instead of one.
So Dr M and an orderly wheel out a general surgery patient — with multiple stab wounds — to first get in the C-sec.
By 8 pm, the ward is overflowing, and patients are now being accommodated in trolleys and stretchers in corridors. Dr M quickly gulps down two more bananas while running in and out of the minor OT. His textbook is always by his side. In the minor OT, doctors use the five minutes or so between cases for a quick read. Dr M’s final year exam is a year away.
At 9 pm, now 12 hours after his duty started, he is preparing for his third major case of the day. A patient has come in bleeding with multiple cuts on his wrist — a suspected suicide attempt. However, a case of ruptured ectopic pregnancy — a pregnancy in the Fallopian tube instead of uterus — arrives just then. The gynaecologists need a general surgeon to assist them, but Dr M’s seniors need him in the suicide attempt case too. So while the gynaecology resident doctor argues with the sister in charge of the OT, Dr M finishes his case in 25 minutes.
Doctors, nurses, anaesthetists are all ready for the ectopic pregnancy now, but they have to wait half an hour for the mobile ECG machine and its technician. Two hours later, at around 1 am, the patient is finally out. But the foetus could not be saved.
Dr M’s next two hours are taken up by a household burns patient. At around 4 am, a six-year-old child who has gulped two beads is brought in. Dr M had been preparing a urology case who had been waiting six hours for his turn in the OT, but again, a child gets priority.
Next, around 5 am, a 13-year-old is wheeled in. She fell from the roof of her house two hours earlier and has already been to three government hospitals. Neurosurgery residents have operated on her concussion but there are multiple wounds in her abdomen and face. With her liver and spleen both ruptured, Dr M and his senior have to take over.
As he emerges from the OT at 7.30 am, Dr M conceals a yawn. He is thinking about his first meal in nearly 24 hours. However, the nurse catches him just as he is cleaning his hands. One of the patients he catheterised in the afternoon has a leak in the urine bag again. A senior calls him to also check on a pancreatitis patient who was brought in during the night.
At 8 am, Dr M is preparing for his next duty shift, finishing the last of his bananas, when he is again summoned. A patient with symptoms of twisting in his testes had arrived with acute pain at 3 am. Doctors needed a colour doppler test to determine if the testes was retrievable, and the patient had been sent to AIIMS. He had now come back with the tests done at a private centre.
By the time doctors finish on him, it is 10 am and Dr M is late for his next shift. It is OT day, his favourite, and he skips the meal he had been longing for. Instead, Dr M heads to the emergency duty room’s washroom to freshen up. It has not been cleaned as usual. With eight hours of OT without a break ahead of him, Dr M ignores the last patient who needs suturing — telling the nurse to wait for the next shift — and hurries out. He drives to a nearby coffee shop and, while his coffee is coming, uses the washroom there.
In 10 minutes, he is back in the car. By the time he is back at hospital, he is an hour late for his shift.
The next seven hours are spent in the OT. Till 5 pm, he assists a consultant on six cases. At 5.15 pm, Dr M sneaks out to the hostel canteen. He has been told his unit head wants to do a round of the wards before he calls it a day, and he has just about time to gulp down four bhaturas with lassi — his first meal in 34 hours. He usually has dinner between emergency cases, but last night was too busy.
Through the 15 minutes of his meal, he leafs through his Sabiston to read up on torsion (twisting) of the testes. By 5.40 pm, Dr M is back with his consultant.
At 8 pm, Dr M is finally off duty. For 12 hours, till his shift in the OPD the next day.
Back to Sabiston, he smiles.


